Introduction
Globally, it is estimated that 11 percent of births are given by adolescent girls of age 15-19 annually, and95 percent of these births are in low-income countries[1]. Each year, about 210 million women around the world become pregnant. Among them, about75 a million pregnancies (36%) are unplanned and or unwanted [2]. Unplanned or unwanted pregnancy is one of the leading causes of maternal mortality and morbidity in South Asia. For example, 30% of pregnancies in Bangladesh, 21% in India, 35% in Nepal are unplanned [3]. World Health Organization(WHO) estimated an annual twenty-two million unsafe abortions happen globally, almost all of which take place in developing countries [4]. About 14% of unsafe abortions in developing countries are among women under 20 years [3].
After the legalization of abortion in 2002, Nepal has made significant progress in providing safe abortion care services to Nepali women by establishing comprehensive abortion care at public sector facilities[5, 6]. However, unsafe abortion remains a public health problem in Nepal. An estimated 14% of maternal deaths at health care facilities were reported due to abortion [7]. Despite the availability of legal abortion services in Nepal, the number of abortions performed outside registered facilities by unregistered providers is estimated to be high. In Nepal, the prevalence of premarital sex has been reported as 39%among college males and 12% among college females. The Nepal Adolescent and Young Adult Survey 2000reported that almost one-fourth of sexually active unmarried young people were involved in risky sexual practice and unexpected opportunity is the most commonly described reason for risky sexual behaviour [2].
The adolescent period is a very crucial period of life,and they are in the transition phase so because of love and curiosity they may involve in sexual intercourse and due to the lack of knowledge and awareness in deciding what is irrational that could force them to adopt many unsafe experiences. Unsafe sex among adolescent predisposes them to unwanted pregnancies, unsafe abortions, and pregnancy-related complications. Complications from unsafe abortion lead to maternal deaths and several other morbidities related to abortion worldwide, placing high risk and leading to severe physical, psychological, and financial consequences for adolescent girls [8]. The adolescent in rural areas are less informed, less experienced for accessing reproductive health services. Rural adolescents often lack basic health information, knowledge and access to affordable, confidential health services for reproductive health [9]. Considering the importance of adolescent ’s health in preventing unintended pregnancy and unsafe abortion, this study aimed to assess the level of awareness on safe abortion among adolescent girls in a rural area of the Mahottari district of Nepal.
Methods
The study design was community-based cross-sectional and study was carried out in rural areas of Mahottari district, Province 2 of Nepal between January and March 2019. The study population includes adolescent girls aged 10 to 19 years living inBardibas municipality of Mahottari district province2 of Nepal. The total population of the municipality was 66358 [10], and the district was 627,580 [11]. Adolescent girls who gave consent for the study were included in the study. Adolescent girls who were physically or mentally ill and unable to participate in the study were excluded from the study.
The sample size and sampling procedure sample size was calculated by using the formula n = z2pq/d2. Where, z is the standard normal distribution equals 1.96 at 95% confidence level and is the percentage of adolescent girls who think abortion is legal in Nepal (42.1%) taken from NepalDemographic and Health Survey 2016 [12, 13]. Considering 5% of permitted error, the sample size came to 374. Assuming 10% of non-response, the final sample size was determined as 412.
Multistage random sampling was adopted. First, Bardibas municipality was selected randomly out of five municipalities in Mahottari district. Second,from the selected municipality, three rural wards were selected randomly. Third, the list of households and the adolescent population in the wards was obtained from the office of the municipality. All the households were numbered serially, and households were selected by use of a systematic random sampling procedure.Then, the adolescent girls were selected from selected households. If there were more than one adolescent girls in one house, then one respondent was selected by the use of the simple random technique.
Data collection, mining and analysis data were collected from respondents by face to face interviews using a semi-structured questionnaire adapted from Nepal Demography and Health Survey2016 [13] and other studies [14, 15]. Pretesting ofthe questionnaire was done in a similar population of the neighboring municipality (Bijalpura village)with 10% samples, and modification was done where necessary. Raw data was checked on the spot to detect errors and corrected on the same day to make sure that the data were accurately filled. The collected data were processed and analyzed by using different descriptive and analytical, statistical methods.
Scoring of the awareness responses from the questionnaire:
Assessment of awareness among adolescent girls was assessed based on the following fifteen major parameters on safe abortion (Supplementary file 1).One score (0 or 1) was assigned for each parameter by asking the respondents for their awareness regarding abortion. For awareness, we assigned score 0 for each of the incorrect response and scored 1 for each of the correct response. As the score of these parameters ranged between 0 and 1, the total possible maximum score is 15 for awareness on safe abortion. The sum ofscores for all the parameters for each participant was calculated and taken as the level of awareness. The median for awareness was calculated. The total scores for each respondent were then split in the median.If the correct responses were more than the median score, the respondents’ awareness was considered“High.” If the correct responses were less than orequal to the median, the awareness was considered“Low” [13, 16, 17].
Age of Adolescent girls was categorized as, 10-13 years, 14–16 years, and 17-19 years. Education was recorded as primary or lower secondary and secondary and above. Ethnicity/caste was based on the caste system in Nepal and was divided into three major groups based on available literature and similarities between the caste/ ethnic groups: upper caste (Brahmin, Chhetri, and Rajput and non-dalitterai caste group like Yadav, Koiri, Sudi/Teli), Adibasi/Janajati and Dalit. Religion was categorized as Hindu and Muslims/others (Christian, Boudha). Types of family categorized as nuclear and joint. Marital statuswas coded as married and unmarried. Family monthly income was recorded as, less than 10,000, between10,000 to 20,000 and more than 20.000 in Nepali currency. Awareness in terms of high and low category was taken as the dependent variables. Age, caste, religion, education, marital status, types of family and family income was taken as explanatory variables.
Statistical Analysis
The association between independent variables and the level of awareness among adolescent girls was examined using univariate logistic regression analysis. Then, the effect of each of the explanatory variables was adjusted for all other variables together in a multivariable logistic regression model. All the significant factors (p<0.05) in the univariate logistic regression analysis were included in the multivariable logistic regression analysis with backward elimination methods. Data were analyzed using Statistical Package for Social Sciences Version 23.0 for Windows.
Ethical approval was obtained from ethics committee of Janaki Medical College, Janakpur, Nepal (Approval number: 23-2075/2076). Informed consent was taken from the participant and confidentiality was maintained.
Results
Out of 412 respondents, most of the respondents(44.2%) were from age group 17 to 19 years Majority of respondents (91.3%) were from Hindu community and (71.8%) belong to the upper and non-Dalit teraicaste group. Furthermore, 89.1% of the respondents were unmarried and more than half (51.2%) of the respondents had secondary and higher education.More than half (57.8%) of respondents belong to joint family and forty-three percent of the respondents had monthly income in Nepali rupees of between the groups 10,000-20,000.
After summing all the points obtained (out of a possible total of 15) for awareness on safe abortion,the maximum score obtained was fourteen points and the minimum was five points. The mean was 9.6 and the median was 10.0. Among all (412) adolescent girls,88 (21.4%) were categorized as having very low level of awareness about safe abortion (5 to 7 points), 136(33.0%) had low level of awareness (8 to 10 points)and 188 (45.6%) had high level of awareness (11 to 14points). In summary, just over half of the adolescent girls (54.4%; 224) had low level of awareness regarding safe abortion and (45.6%; 188) presented high level of awareness. Categorizing the level of awareness regarding safe abortion as low (≤median;10 points) and high (>median; 11 to 14 points), the associations between level of awareness about safe abortion and the adolescent socio-demographiccharacteristics is presented in table 1.
Table 1. Association of Socio-demographic Characteristics and Awareness on Safe Abortion among adolescent girls.
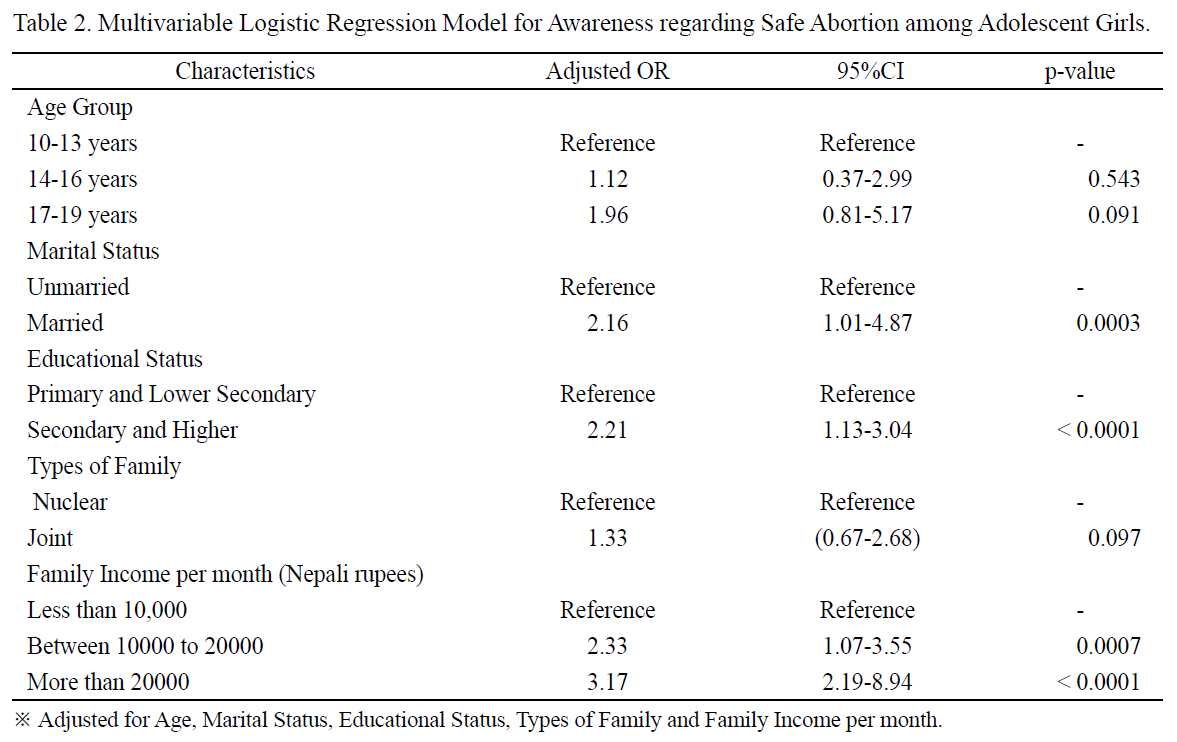
The result of the multivariable analysis is shown inTable 2. In our study, we found no evidence of any association between level of awareness about safe abortion with age and types of family of the adolescent girls in multivariable analysis after adjusting potential confounders. However, marital status, educational status and family income were significantly associated with level of awareness on abortion among of the adolescent girls. The odds of higher awareness amongthe married adolescent were 2.16 times (AOR=2.16;95% CI: 1.01-4.87) greater than unmarried adolescent whereas the odds of higher awareness among the adolescent girls who had education of secondary level and higher were 2.21 times (AOR=2.21; 95%CI:1.13-3.04) more than those who had primary or lower secondary level of education. Similarly, the adolescent girls who had a monthly family income of 10,000-20,000 and more than 20,000 were 2.33 times (AOR =2.33; 95% CI: 1.07–3.55) and 3.17 times (AOR = 3.17;95% CI: 2.19–8.94) more likely to have high aware regarding abortion than those who had family income of less than 10,000 per month.
Table 2. Multivariable Logistic Regression Model for Awareness regarding Safe Abortion among Adolescent Girls.Discussion
 Discussion
Discussion
The study identified the most important issues on in adolescent health. Nepal made abortion legal in September 2002. The government began providing comprehensive abortion care services in March 2004.The abortion law allows women to terminate their pregnancy under the following three conditions: (i)pregnancies of 12 weeks’ gestation or less for any woman according to her own decision, (ii) pregnancies of 18 weeks’ gestation if the pregnancy is a result of rape or incest, and (iii) pregnancies of any duration with the recommendation of an authorized medical practitioner if the life of the mother is at risk, if her physical or mental health is at risk, or if the fetus is deformed. However, the law prohibits abortions done without the consent of the woman, selective sex abortions, and abortions performed outside the legally permissible criteria [13, 18].
The current study identified less than one fourth ofthe adolescent girls had very low level of awareness having score 5 to 7 points, one-third of the adolescent girls had low level of awareness with score 8 to 10points and less than half of the adolescent girls had high level of awareness having a score between 11 to14 points out of 15 points. Moreover, the study found that only 45.6% of adolescent girls had high level of awareness regarding safe abortion. This study revealed a comparatively higher proportion of adolescent girls who had a higher level of awareness regarding safe abortion than that of studies conducted in Nepal [13],India [16], Latvia [19] and Zambia [20], but lower than the studies from Nepal [21], Ethiopia [22] and India [23]. However, the finding is supported by the several other studies from Nepal [14] and India [24]. These disparities in the study might be because of differences in the educational level among adolescent girls.
Our finding showed two times higher odds of awareness among married adolescents than an unmarried adolescent. In concurrent with the current study, other several studies, [14, 25, 26] have described the association between the marital status of women and level of awareness regarding safe abortion. This shows sever-married women were more aware regarding safe abortion where never-married women expected more negative responses from having a safe abortion.
In this study, adolescent girls who had an education of secondary level or more had a higher level of awareness on safe abortion than those who had a primary or lower secondary level of education. Thefinding is line with other studies [13, 25, 27, 28] that showed that a higher level of education is positively associated with a higher level of awareness on safe abortion.
The adolescent girls who had a monthly family income of 10,000-20,000 and more than 20,000 were2.33 times and 3.17 times more likely to have high aware regarding safe abortion than those who had a family income of less than 10,000 per month.The finding is concurrent with the findings of the other studies [13, 22, 25]. Thus, the study identified marital status, level of education and monthly family income are important factors associated with the level of awareness regarding safe abortion among adolescent girls in rural areas of the Mahottari district of Nepal.
Limitation of study
The study was based on only adolescent girls who were present in the study area at the time of the survey,so it may not be truly representative of all adolescent girls of Mahottari district. All the responses were self-reported therefore the result may bias. The study was conducted within a limited time period.
Summary
This study aimed to assess the level of awareness on safe abortion among adolescent girls in rural area of the Mahottari district of Nepal. A community-based cross-sectional study was conducted in rural areas of Mahottari district of Southern Nepal between January and March 2019.A sample of 412 adolescent girls was selected using multi-stage cluster sampling.A multivariable logistic regression model was adapted to explore level of awareness among adolescent girls.This study found that 45.6% of adolescent girls had high awareness regarding safe abortion. The odds of awareness among the married adolescents was higher(AOR=2.16; 95% CI: 1.01-4.87) than unmarried adolescent whereas the odds of awareness among the adolescents who had education of secondary level and more had higher (AOR=2.21; 95%CI: 1.13-3.04) than those who had primary or lower secondary level of education. Similarly, the adolescents who had a monthly family income of Nepalese Rupees (NRs.), 10,000-20,000 and more than NRs. 20,000 were respectively,2.33 times (AOR = 2.33; 95% CI: 1.07–3.55) and3.17 times (AOR = 3.17; 95% CI: 2.19–8.94) more likelihood to have high awareness regarding safe abortion than those their counterparts. The study showed that the overall level of knowledge towards safe abortion was found low. Socio-demographic factors like marital status, level of education, and family income were the factors independently associated with level of awareness on safe abortion. Therefore, efforts should be exerted towards arising and improving the awareness of abortion care which may reduce unwanted pregnancy, abortion and other complications related to abortion.
References
- Mangiaterra V, Pendse R, McClure K, Rosen J. Adolescent pregnancy. Department of making pregnancy safer(MPS). 2008;1
- Adhikari R. Factors affecting awareness of emergency contraception among college students in Kathmandu, Nepal. BMC women's health 2009;9(1):27 https://doi.org/10.1186/1472-6874-9-27
- Subedi S. Knowledge, attitude and practices of emergency contraception among youths of Parbat District. JHAS. 2012;2(1):50-3 https://doi.org/10.37107/jhas.77
- World Health Organization. Safe Abortion: Technical and Policy Guidance for Health Systems, Geneva: WHO, 2012. Available from: http://appswhoint/iris/bitstream/10665/70914/1/9789241548434_engpdf.2012
- Thapa S. Abortion law in Nepal: the road to reform. Reproductive Health Matters 2004;12(sup24):85-94 https://doi.org/10.1016/S0968-8080(04)24006-X
- Samandari G, Wolf M, Basnett I, Hyman A, Andersen K. Implementation of legal abortion in Nepal: a model for rapid scale-up of high-quality care. Reproductive health 2012;9(1):7 https://doi.org/10.1186/1742-4755-9-7
- Pradhan A, Suvedi B, Barnett S, Sharma SK, Puri M, Poudel P, et al. Nepal maternal mortality and morbidity study 2008/2009. Family Health Division, Department of Health Services, Ministry of Health and Population, Government of Nepal, Kathmandu, Nepal. 2010
- Ahman E, Shah I. Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008. 2011
- Tegegn A, Yazachew M, Gelaw Y. Reproductive health knowledge and attitude among Adolescent : a community based study in Jimma Town, Southwest Ethiopia. Ethiopian Journal of Health Development 2008;22(3)
- Education in Figures 2017 (At a glance). Ministry of Education, Science and Technology, (Statistics, Policy and Research Section), Governemnt of Nepal, 2017
- Central Bureau of Statistics Nepal. National Population and Housing Census 2011 (National Report). Kathmandu, Nepal: Government of Nepal National Planning Commission Secretariat Central Bureau of Statistics Kathmandu, Nepal; 2012
- Israel GD. Determining sample size. 1992
- Ministry of Health and Population, New ERA, ICF International. Nepal Demographic and Health Survey 2016 Kathmandu, Nepal and Rockville, Maryland, U.S.A.: Ministry of Health and Population, New ERA and ICF International; 2017
- Andersen KL, Khanal RC, Teixeira A, Neupane S, Sharma S, Acre VN, et al. Marital status and abortion among young women in Rupandehi, Nepal. BMC women's health 2015;15(1):17 https://doi.org/10.1186/s12905-015-0175-4
- Sjostrom S, Essen B, Syden F, Gemzell-Danielsson K, Klingberg-Allvin M. Medical students' attitudes and perceptions on abortion: a cross-sectional survey among medical interns in Maharastra, India. Contraceptio 2014;90(1):42-6 https://doi.org/10.1016/j.contraception.2014.02.005
- George RR, Devendraakhilesh P, Iahmo T, Moray KV, Cherian AG, Prasad JH. Why are abortions the answer? Prevalence, knowledge and attitude towards induced abortions among women attending a secondary level health care facility in Tamil Nadu, Southern IndiaInternational Journal of Community Medicine and Public Health 2017;4(2):532-6 https://doi.org/10.18203/2394-6040.ijcmph20170286
- Acharya D, Singh JK, Adhikari S, Jain V. Associat ion between sociodemographic characteristics of female community health volunteers and their knowledge and performance on maternal and child health services in rural Nepal. Journal of multidisciplinary healthcare 2016;9:111 https://doi.org/10.2147/jmdh.s98700
- Ministry of Health and Population. Annual Report, 2016/2017. In: Service DoH, editor. Kathmandu, Nepal: Department of Health Services; 2018
- Melgalve I, Lazdane G, Trapenciere I, Shannon C, Bracken H, Winikoff B. Knowledge and attitudes about abortion legislation and abortion methods among abortion clients in Latvia. The European journal of contraception & reproductive health care 2005;10(3):143-50 https://doi.org/10.1080/13625180500332224
- Cresswell JA, Schroeder R, Dennis M, Owolabi O, Vwalika B, Musheke M, et al. Women's knowledge and attitudes surrounding abortion in Zambia: a cross-sectional survey across three provinces. BMJ open 2016;6(3):e010076 https://doi.org/10.1136/bmjopen-2015-010076
- Tuladhar H, Risal A. Level of awareness about legalization of abortion in Nepal: A study at Nepal Medical College Teaching Hospital. Nepal Med Coll J 2010;12(2):76-80
- Bitew S, Ketema S, Worku M, Hamu M, Loha E. Knowledge and attitude of women of childbearing age towards the legalization of abortion, Ethiopia. J Sci Innov Res 2013;2(2):2320-4818
- Bobhate P, Shrivastava S. A cross sectional study of knowledge and practices about reproductive health among female Adolescent in an urban slum of Mumbai. Journal of Family and Reproductive Health 2011:117-24
- Mittal K, Goel MK. Knowledge regarding reproductive health among urban adolescent girls s of Haryana : official publication of Indian Association of Preventive & Social Medicine. Indian journal of community medicine 2010;35(4):529 https://doi.org/10.4103/0970-0218.74374
- Thapa S, Sharma SK, Khatiwada N. Women's knowledge of abortion law and availability of services in Nepal. Journal of biosocial science 2014;46(2):266-77 https://doi.org/10.1017/S0021932013000461
- Johnston HB. Abortion practice in India: a review of literature: Centre for Enquiry into Health and Allied Themes Mumbai; 2004
- Reichelt PA, Werley HH. Contraception, abortion and venereal disease: Teenagers' knowledge and the effect of education. Family Planning Perspectives 1975:83-8
- Kavanaugh ML, Bessett D, Littman LL, Norris A. Connecting knowledge about abortion and sexual and reproductive health to belief about abortion restrictions: findings from an online survey. Women's Health Issues 2013;23(4):e239-e47 https://doi.org/10.1016/j.whi.2013.04.003